Short-term constipation or intermittent bouts of constipation are unlikely to cause any long-term problems. Sometimes a split or tear in the anal skin (an anal fissure) can occur with the passage of particularly big or hard stools (faeces). This is very painful and there may be a small amount of fresh red blood on tissues
Long-term or persisting (chronic) constipation and long-term use of laxatives can result in your bowel becoming sluggish and ‘lazy’. This means that the bowel doesn’t work very well on its own, without medication. Constipation then becomes a vicious cycle and even more chronic. Try to avoid getting into this situation in the first place by using laxatives for short periods of time only. Consult your GP for advice if you are needing them regularly. Some people with persistent and severe constipation do require regular laxatives.
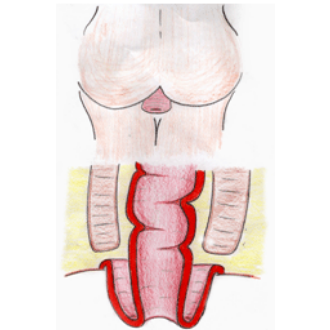
Severe chronic constipation can sometimes result in faecal impaction. In this condition, a large mass of hard faeces blocks the rectum. The mass is too big to pass and the rectum is stretched and enlarged, so the muscles within it don’t work so well and are unable to push the faeces out. Sometimes people with this problem think that they have diarrhoea. This is because liquid faeces, from above the blockage, leak around the hard lump of faeces and out of the anus. This is known as overflow diarrhoea. In this situation, you may also have faecal incontinence – that is, you have no control over this liquid faeces leaking out. Faecal impaction with overflow diarrhoea is likely if you have been getting progressively more constipated, and then have liquid faeces, possibly explosive, and without much control. If a doctor or nurse examines the anus, the hard faeces can often be felt, confirming the diagnosis. The diagram below shows this process:

In order to treat impaction, higher doses of laxatives need to be used, and sometimes enemas or suppositories. Temporarily, symptoms of diarrhoea may worsen but it is important to keep up with treatment, to clear the blockage. After the large mass of faeces is cleared, laxatives are often needed for a while (or perhaps even long-term or intermittently) to prevent the problem recurring.